Dependence on substances is complex and a condition that often proves difficult to manage. Much remains to be understood about the processes involved yet, in recent years, advances – especially in the brain sciences – have provided further understanding of the processes involved and it is hoped that, through these insights, new and innovative treatment strategies will become available.
DEFINITIONS
Definitions are complex and important in this field. Original terms can evolve to stigmatise individuals and communities yet need to be used by professional and academics to ensure clarity of meaning. The word ‘addict’, for example, is no longer widely used. It is derived from the Latin verb addicere, which means ‘to assign’. It was used as a legal term in the 16th century as someone bound over to another person: the implication being that freewill has been taken away and handed over to another
In most cultures there exists a moral dimension and an expectation that the individual is failing to exercise free choice. This is the “choice model” of addiction. The choice model is less prominent today as addiction is increasingly viewed as a disease of the brain – the “disease model”. Lastly there is the “self-medication model” in which people use drugs to modify painful emotions and memories. There is some validity for each of these models in the life experiences of people who use drugs. Initially, drug use may be experimental and certainly at this stage involves some element of voluntary choice, but then a point is reached where the individual’s ability to choose is rendered powerless.
THE JOURNEY TO DEPENDENCY
Patterns of mood-altering drug use form a fivestage continuum: appropriate use, misuse, experimental use, abuse and psychological and/or physical dependence (addiction). Appropriate use of a drug is when it is taken for its medical indication, at the right dose and for the right period of time. Misuse occurs where the drug is used, for example, for its mood-modifying properties rather than its analgesic effect – as in the case of codeine – but is still used within the recommended dose. Experimental use is the conscious use of the drug to modify mood. In misuse, the drug is taken for a purpose other than its medical indication, at a dose higher than indicated and for longer than recommended.
Misuse clearly refers to the use of any illicit drug that can result in physical, psychological, economic, legal and social harm, either to oneself and/or others, although the term can also be applied to prescribed drugs.
Misuse begins generally as experimental use. Psychological and/or physical dependence occurs following habitual use, with high potential for dependency.
Dependency is characterised by:
• The need to take a drug to experience its pleasurable effects
• Behavioural or personality changes resulting from abrupt discontinuation
• The need to increase the dose and frequency to sustain its initial effect (tolerance) Psychological dependence is an emotional state that craves (desires) the drug for either its positive effect on mood, or to avoid the negative effects of withdrawal. All mood-altering drugs can create psychological dependency.
Cocaine, for example, produces little physical dependence but is highly psychologically reinforcing. Physical dependence occurs where the body is unable to function properly without the drug and withdrawal symptoms occur.
The following short definition is close to current thinking on drug addiction:
“A compelling desire to take a substance or engage in a behaviour and to prioritise this above other things.”
Addiction services currently use the term Substance Use Disorder as a people-first term which helps reduce the stigma suffered by many of those who enter treatment. In this article, written for a professional audience, we will mainly use the term Drug Dependence/dependence and substance use disorder interchangeably.
DRUG HARMS AND RISKS TO INDIVIDUALS AND OTHERS
Drugs that alter mood always have the potential to produce dependency.
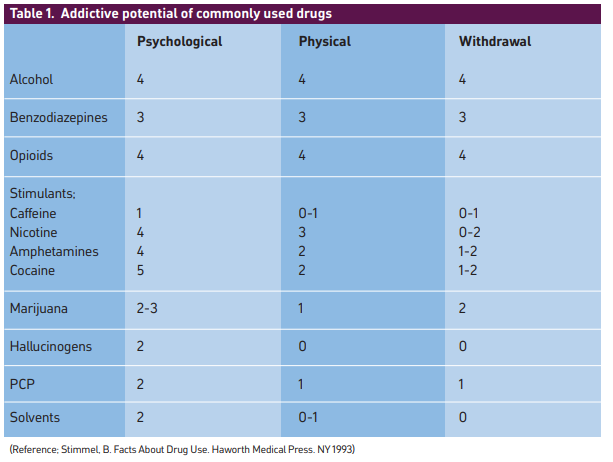
Table 1 outlines some common drugs with the potential to cause psychological dependence, physical dependence and withdrawal. Each parameter is reported on a scale of 0 to 5, where 5 indicates the highest degree of addiction.
NEUROTRANSMITTERS AND DEPENDENCE
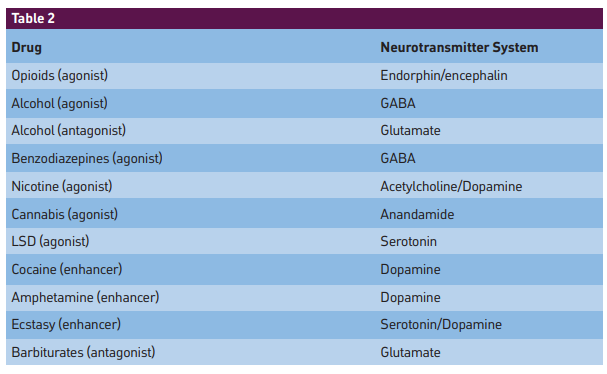
Drugs elicit their psychoactive effects via disruption of endogenous neurotransmitters. They do this by: (1) mimicking the activity of an endogenous neurotransmitter (agonist); (2) increasing the endogenous transmitter release (enhancer); (3) by blocking a natural transmitted (antagonist). Table 2 lists neurotransmitter systems affected by drugs of dependence.
Generally, the more effective a drug is in producing its CNS pharmacological effect, the more specific it interacts with a receptor and the greater its potential for dependence. Drugs with a lower efficacy are usually partial-agonists and can be useful in maintenance treatment since they provide some reinforcement, yet have a much less pronounced effect, allowing someone addicted to the agonist to more easily come off the drug when switched to the partial-agonist. For example, buprenorphine is a partial-agonist for opioid receptors and is used as substitution therapy in opioid dependency. The knowledge that alcohol also acts via the GABA and glutamate receptor systems allows development of acamprosate which acts at these sites and is helpful in managing patients with alcohol dependency.
Naturally glutamate receptors stimulate awareness and over-stimulation brings about stress and anxiety. Antagonists for these receptors – alcohol and barbiturates for example – produce a positive psychological effect. But antagonists that block neurotransmitter effects at other sites, for example, naltrexone at opioid receptors will precipitate withdrawal in people who use opioids. .
SPEED OF DELIVERY
The pharmacokinetics of a drug, a characteristic of the drug or its pharmaceutical form, can contribute significantly to its potential for dependence and/or misuse. In general, the faster a drug enters the brain, the more reinforcing it is (onset of action). Formulation of a drug can be manipulated to improve the speed of delivery to the brain. Cigarettes, for example, are more dependent forming compared to cigars, pipe tobacco and chewing tobacco. Cigarettes are manipulated so that the nicotine in the smoke is alkaline and therefore cannot be absorbed in the mouth. The smoker is required to inhale where the huge surface area available in the lung and the lipophilic nature of nicotine allows rapid transport across the lung wall into the blood and rapid delivery to the brain (in about seven seconds). Nicotine replacement therapy (NRT) formulations are designed to deliver nicotine less rapidly and not reinforce the brain effects of nicotine.
In a similar way, people who use opioids prefer heroin over morphine because it is more lipophilic and enters the brain faster. Cocoa leaves are chewed but seldom cause dependence, whereas cocaine is addictive on long-term use, However, “crack” cocaine – the free base salt – is most rapidly absorbed when smoked and, as a result, is highly addictive.
The half-life of the drug is also important. Shortacting drugs, where the receptor is frequently occupied and freed-up, are more likely to lead to withdrawal symptoms and dependence. Patients wishing to withdraw from benzodiazepines are switched to a longer acting version (diazepam) before stepping down. The same principle applies in opioid dependency, where the individual is placed on methadone or buprenorphine with a much longer half-life than morphine and heroin. These are also taken orally to ensure the onset of action is longer versus injecting or smoking (although a long-acting buprenorphine injection is now available in the UK).
DOPAMINE AND ADDICTION
All drugs of misuse, irrespective of the receptor system they act on, produce positive/altered mood effects through a direct or indirect release of dopamine in either the nucleus accumbens or the pre-frontal cortex. Cocaine and amphetamines release dopamine directly, whereas opioids switch off the firing of GABA neurons that inhibit dopamine.
Research has clearly indicated a central role for dopamine in the initiation of addiction and there is speculation that some variations of the dopamine receptor gene may explain why some individuals are more prone to dependent drug-use compared to others, and why this may have genetic implications that dependency runs in families. Where dopamine is over-stimulated by drug use, on withdrawal, a dopamine “crash” is experienced, manifesting in a very low, negative mood. Some drugs that block dopamine re-uptake such as desipramine are used to treat cocaine withdrawal and dopamine over-activity, probably underlying alcoholic delirium tremens. Haloperidol, a dopamine-D2-receptor antagonist is used to treat it. All these factors place dopamine and the motivational system – of which it is the key neurotransmitter – at the centre of substance use disorders.
THE MOTIVATIONAL SYSTEM
The human brain has evolved a complex motivational system designed to set plans and priorities for the individual, and these are normally to do with survival and reproduction. The motivational system (also known as the reward system) occupies a specific region in the mid-brain and, in theory, this region is in a constant state of flux resulting from the influences within it and the constantly changing internal and external environments.
Psychological and emotional states are the product of neurotransmitters, mainly dopamine, acting within this region. The motivational system is unstable and our past and current experiences significantly affect the system recalibrating what we value as important and what we therefore choose to seek out. This is more pronounced in teenagers whose brains are still forming. Drugs, due to their ability to alter mood by affecting dopamine in the motivational system, hijack the motivational system and in doing so set new priorities and values which are then focused on seeking out drugs and taking them at the cost of ignoring other goals, such as having good relationships or being successful in a career. In short, substance use disorders are a distortion and disruption of the brain’s motivational system. This brain process is closely linked to, and is a part of, how the brain learns. Indeed, a number of current theories of substance use view it as a normal, if extreme and destructive, outcome of the brain’s normal learning processes.
THE ENVIRONMENT AND SOCIAL STATUS
Our environment, our social status and indeed access to psychoactive drugs all play a significant role in determining our risk of developing a substance use disorder. A seminal study from the 1970s on GIs with opioid dependence returning home from Vietnam showed that, when returned to their families, only seven per cent of those with dependence continued with drug use.
The more hostile, depressing and hopeless the environment we find ourselves in, the more likely psychoactive drug use leads to dependence and therefore it follows that those with low social status are most vulnerable. Low social status is a factor that also applies in other primates.
Stress, anxiety, boredom and depression: factors often linked to environment and social status, encourage, when accessible, self-medication with drugs to improve mood. Again this applies to other primates; monkeys housed in particularly depressing environments will voluntarily smoke cigarettes laced with hallucinogenic drugs which they would otherwise avoid.
In his famous Rat Park studies, Bruce Alexander showed rats only became dependent on morphine when forced to live in a sensory deprived environment. Stanton Peele, a scientist working in the field of dependence, maintains that people normally don’t get dependent to the drugs they encounter because they “have something better to do”. It’s not the drug; it’s the brain and the environment the brain is adapting to.
DESIRE VS PLEASURE
People Who Use Drugs (PWUDs) are driven more by desire than by pleasure and dopamine is the neurotransmitter of desire. PWUDs persist with their habit even when it becomes unpleasant and they would dearly wish to quit. Pleasure might be a route into dependence, but it is not what generally sustains it. Also, avoidance of withdrawal might help sustain dependence but, again, it is not the root cause. The main reason is a problem with desire.
TREATMENT STRATEGY
Given these insights to drug dependency, the aim of treatment strategy should include:
(1) Reducing the rewarding value of the drug or behaviour (Opioid Substitute Therapy – OST – such as methadone or buprenorphine).
(2) Strengthening the individual’s voluntary control over their behaviour.
(3) Increasing the reward value of alternative and less harmful sources of pleasure.
(4) Weakening or reversing the long-term change in learning and memory that allow cravings to persist
(5) Reducing exposure to environmental cues associated with the drug.
(6) Reducing the individual’s sensitivity to these cues.
Given the complexity of substance misuse and its subtle interaction of the drug, the brain and the environment, it is perhaps unsurprising that there are poor outcomes from drug dependency interventions, with a high percentage of problem drugs users, who eventually do quit, giving up spontaneously and without much help.
TAKE THE FIVE-MINUTE TEST